
Table of Contents
- The study that turned an unlikely idea into a serious question
- Why alcohol related liver disease is so difficult to treat
- How cannabis might be influencing the liver
- What the numbers do and do not prove
- Why CBD is getting the most attention
- Why the results resonated so strongly
- What comes next in the research
- What this means for patients right now
The study that turned an unlikely idea into a serious question
The new research was led by investigators from Virginia Commonwealth University and VCU Health and examined medical data from more than 66,000 adults across the United States diagnosed with alcohol use disorder between 2010 and 2022. The team then divided participants into three broad categories: those with cannabis use disorder, those who used cannabis without signs of dependence, and those who did not use cannabis at all. Researchers followed the patients for three years after their initial diagnosis to see who went on to develop alcohol associated liver disease, serious liver related complications, or death from any cause. To reduce bias, they used statistical matching methods so that the groups would be more comparable in age, sex, and health conditions.
The results were striking enough to attract wide attention. Compared with non users, patients with cannabis use disorder showed a 40% lower risk of developing alcohol related liver disease. They also had a 17% lower risk of serious liver complications and a 14% lower risk of death from any cause. Even cannabis users without dependence appeared to have a slightly lower risk of developing liver disease than non users, though the strongest associations appeared in the cannabis use disorder group. These are not small numbers, and they help explain why the study spread quickly across health reporting and professional circles. When a large clinical dataset suggests a substantial reduction in disease risk tied to an unexpected factor, researchers pay attention.
But what makes the study especially interesting is that it does not appear out of nowhere. It builds on a growing body of preclinical and mechanistic evidence suggesting that cannabinoids may influence how the liver responds to injury. The authors wrote that preclinical studies have suggested modulation of the hepatic endocannabinoid system, particularly via CBD, may reduce alcohol induced liver injury. In other words, the clinical association they found is not purely random or biologically implausible. There are already lab based reasons to think certain cannabinoids could alter inflammation, oxidative stress, and fat handling in ways that protect liver tissue.
Part of why this study has generated so much interest is the bleak reality of alcohol associated liver disease itself. The condition develops when long term heavy alcohol use overwhelms the liver’s ability to repair and regulate itself. Fat accumulates. Inflammatory pathways stay switched on. Scar tissue forms. At advanced stages, the liver loses the ability to perform basic life sustaining functions such as detoxifying blood, processing nutrients, and producing essential proteins. By the time many patients are diagnosed, they may already be heading toward liver failure or transplant consideration.
The standard medical advice remains reducing or stopping alcohol consumption. That remains the most important step, and nothing in the new study changes that. But the problem is obvious. Many people with alcohol use disorder cannot simply choose to stop and succeed on command. Addiction is not a matter of receiving correct information and suddenly becoming healthy. It is a chronic relapsing condition shaped by neurobiology, trauma, environment, and mental health. That means clinicians have long needed additional treatment tools for the liver itself, not just counseling about alcohol reduction. The VCU researchers framed their work in exactly that context, noting that effective therapeutic options for alcohol associated liver disease remain limited.
This is why an unexpected lead like cannabis compounds can become so important. If there is even a plausible chance that CBD or related cannabinoids could reduce liver injury in heavy drinkers, then the research field has a new direction worth pursuing. Not because cannabis is harmless, and not because association equals cure, but because the unmet need is so large.
How cannabis might be influencing the liver
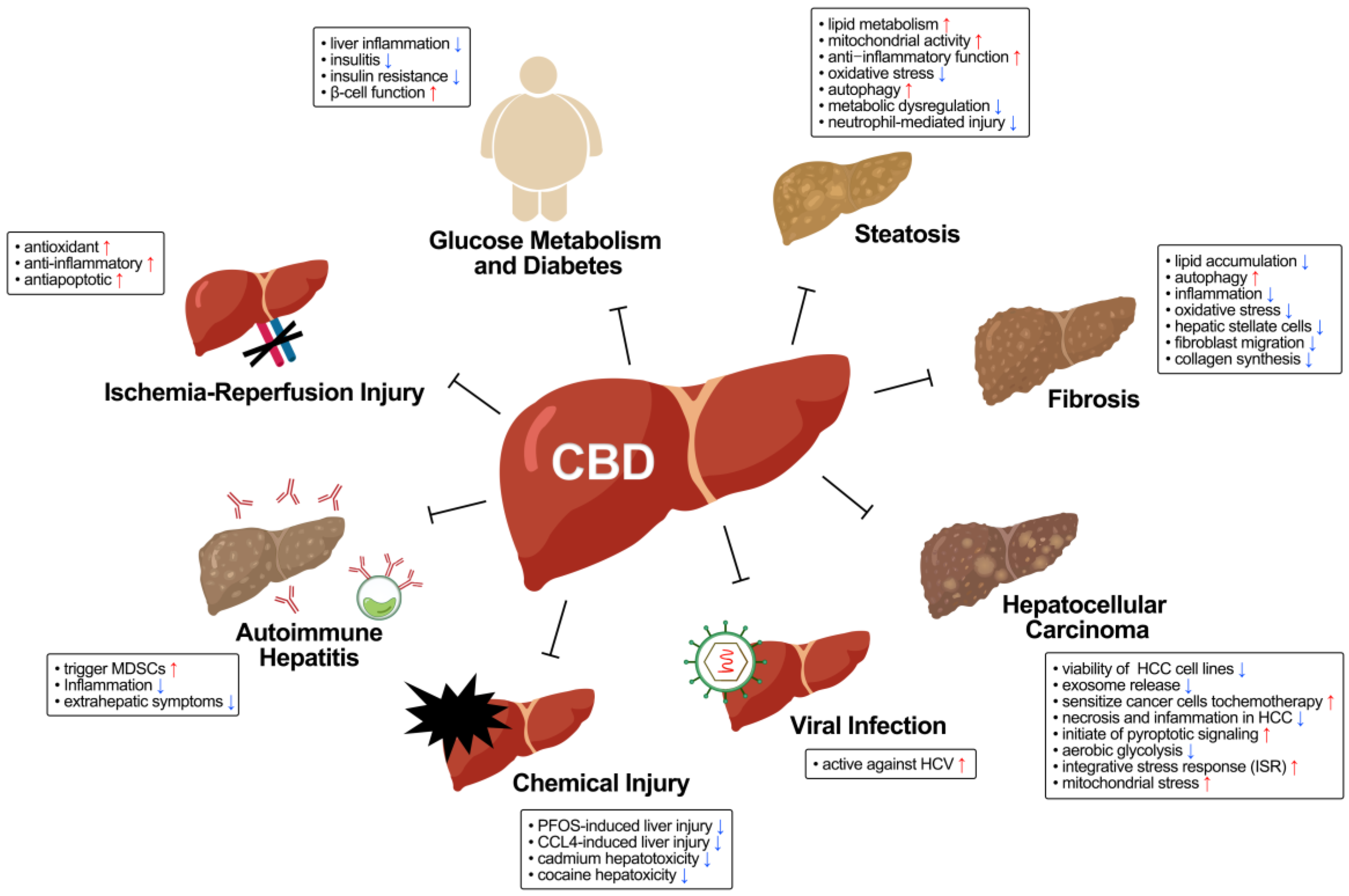
The biological story here is still incomplete, but there are several reasons scientists take it seriously. The liver is connected to the body’s endocannabinoid system, a network involved in metabolism, immune signaling, inflammation, and energy regulation. Preclinical work suggests that cannabinoids, particularly CBD, may reduce alcohol related liver injury through several pathways. These include enhancing mitochondrial activity to improve fat metabolism, reducing oxidative stress, calming inflammatory signaling such as NF-kB and NLRP3 pathways, and influencing fibrogenic pathways involved in liver scarring.
That matters because alcohol associated liver disease is not a single event. It is a cascade. The liver becomes fatty, inflamed, metabolically stressed, and eventually scarred. A compound that can interrupt even part of that cascade might slow or soften the disease process. CBD has been of special interest because unlike THC, it does not produce intoxication and is already used clinically in a very different context for certain seizure disorders. That makes it a more plausible candidate for drug development than a more broadly psychoactive cannabis component. The study’s senior author, Dr. Juan Pablo Arab, said that CBD appears to calm inflammation and reduce some of the chemical signals that drive liver scarring, and that the team’s real world findings may reflect some of those same protective effects in people who drink heavily.
This is where the study becomes more than a curiosity. It begins to connect real patient outcomes with a biologically credible mechanism. That does not prove cause and effect, but it does make the association harder to dismiss.
What the numbers do and do not prove
For all its promise, the study has important limits, and the researchers were unusually clear about them. This was an observational study using medical records, not a randomized clinical trial. That means it can identify associations but cannot prove that cannabis directly caused the lower risk. It is possible that cannabis users differed from non users in ways the researchers could not fully measure, even after statistical matching. They may have had different drinking patterns, different access to care, different diets, or different rates of undiagnosed illness. Observational studies can narrow the possibilities, but they cannot close the case.
Dr. Butros Fakhoury, one of the study authors, emphasized that point directly. He said the study shows an association, not cause and effect, and that researchers still do not know exactly how much, what form, or what dose might be safe or effective. That caution is crucial. Cannabis use carries its own risks, especially for younger people and for those with certain mental health conditions. Smoking cannabis is not the same thing as receiving a carefully dosed pharmaceutical CBD product under medical supervision.
This distinction may be the single most important thing for readers to understand. The study is not telling people with alcohol use disorder to start using cannabis. It is identifying a signal inside a large real world dataset that may point scientists toward future treatments. In medicine, that is a meaningful step, but it is not the same as clinical guidance.
Why CBD is getting the most attention
Among the many compounds in cannabis, CBD has emerged as the most medically plausible candidate for further liver research. One reason is practical. CBD does not intoxicate people in the way THC does, which makes it easier to imagine in a therapeutic setting. Another is regulatory. CBD is already approved by the US Food and Drug Administration for some seizure disorders, which means there is already a foundation of data and clinical experience surrounding its use, although not in people with alcohol associated liver disease.
That said, even CBD is not simple. Fakhoury noted that one major challenge lies in identifying a safe and appropriate dose because CBD itself is metabolized in the liver. For patients with chronic liver disease, that detail becomes especially important. A compound being potentially protective in one context does not mean it is universally safe in every dose or for every patient. That is exactly why the next phase of research must be controlled clinical trials rather than public experimentation or internet driven self treatment.
Still, this is where the study becomes especially intriguing. Many observational findings lead nowhere because the biology is weak or the candidate molecule is not practical. Here, the candidate compound is both biologically plausible and already medically recognizable. That does not guarantee success, but it raises the stakes of future research considerably.
Why the results resonated so strongly
Part of the public reaction to this study comes from the unusual source of the possible benefit. Cannabis is still culturally and politically loaded. For decades it was discussed primarily through the lens of intoxication, criminal law, and culture war. Even in more recent years, as medical and recreational legalization spread, public debates have often swung between overenthusiastic claims and overcautious fear. So when a respected academic group suggests that cannabis related compounds might help protect the liver from alcohol damage, the finding immediately captures attention because it cuts across old assumptions.
There is also a more practical reason the story spread. Alcohol and cannabis are two of the most widely used psychoactive substances in the United States, and liver disease is a major public health burden. A finding that seems to connect all three is bound to draw both hope and confusion. People understandably want to know whether the result applies to them, whether cannabis use is suddenly “good” for the liver, or whether CBD supplements might help. The responsible answer, at least for now, is much more restrained. The study suggests a research lead, not a do it yourself medical plan.
What comes next in the research

The authors and VCU’s public summary both point in the same direction. The next step is to study specific cannabinoids, particularly CBD, in controlled clinical trials. That means giving defined formulations to carefully selected patients, monitoring liver outcomes, watching for side effects, and determining whether the observed association survives under experimental conditions. It also means figuring out dosage, duration, and which patients might benefit most.
If those trials confirm a benefit, the implications could be significant. Alcohol associated liver disease currently has few targeted therapies, so even a modestly effective CBD based intervention could change practice for a large and vulnerable patient population. It could also broaden scientific understanding of the hepatic endocannabinoid system and how it might be manipulated therapeutically in other forms of liver injury.
But clinical trials may also produce less dramatic results than the observational data suggest. That is not failure. That is how medicine works. Strong observational signals are tested, refined, and sometimes narrowed into smaller but still useful truths.
What this means for patients right now
For now, the most responsible interpretation is cautious optimism. The study offers a credible and interesting clue that cannabinoids, especially CBD, might one day become part of alcohol associated liver disease treatment. It does not justify starting cannabis to “protect” the liver. It does not tell patients to replace standard medical care. And it certainly does not cancel out the damage of heavy alcohol use.
What it does do is challenge the idea that the therapeutic possibilities for alcohol related liver disease are exhausted. That alone is valuable. Patients with alcohol use disorder and liver injury often face stigma on top of illness, and treatment innovation in this space can lag behind need. A study like this suggests there may still be unexplored pathways worth following, even in places medicine once overlooked or dismissed.
In the end, the most important thing about this cannabis liver study is not that it offers a miracle. It is that it offers a direction. In a field where options remain limited and outcomes can be devastating, even a well grounded clue matters. The question now is whether future trials can turn that clue into something patients can safely and reliably use. Until then, the finding stands as one of the more surprising and potentially important liver research stories to emerge in recent months.